Needling
Use a 22G cannula (24G in neonates)
Target depth: 1-2 cm
Remove gel at insertion point
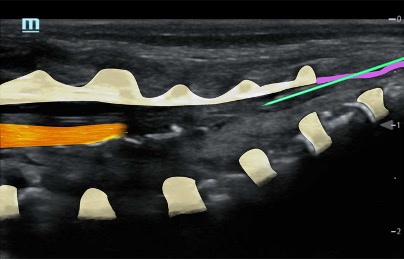
Needle insertion at the apex of the sacral hiatus at an angle of 45⁰ until resistance
Reangle to 30⁰ and insert another 5mm (advance under US vision) – characteristic pop through ligament
Then slide the cannula off the needle (it should slide off easily)
Remove needle, open cannula to air and observe for blood or CSF, then aspirate with a 2ml syringe
Perform saline test à Confirm position (saline expands the epidural space and pushes the dura more anteriorly)
NOTE: If the injectate is not visualised, the LA might be going intravascular or outside of the caudal canal; STOP and reposition the needle.
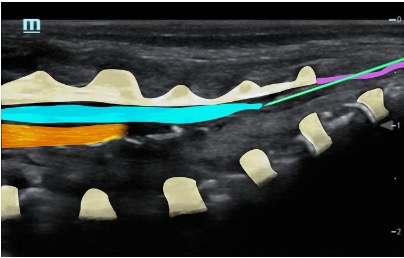
Slowly inject LA and observe spread (aspirate repeatedly)
Levobupivacaine 0.25% max 1ml/kg (+/- clonidine 1mcg/kg for increased duration)
Track the LA spread by sliding the probe cranially (probe positioned paramedian longitudinally); ensure the appropriate level is reached for the intended operation
NOTE: Level of the block will correlate to injected volume
NOTE: For neonates 0.125% levobupivacaine is effective and allows a greater volume to be injected should a higher level be desired (and an alternative technique e.g. direct thoracic epidural or caudal catheter is considered less appropriate)
NOTE: Caution with the use of adjuncts in neonates – clonidine will prolong the block but can cause an increased risk of apnoeas, particularly in premature neonates
Paediatric Plan A Blocks
About
News
Education
Courses
Research
Resources
Grants
Webinars
ASM
Members
Plan A
Plan A Paeds
Plan A Block Videos
Terms & Conditions
Privacy
ASFRA/RAUK Meeting 2026
13th annual conference of the African Society of Regional Anesthesia & Pain Therapy
Membership Terms and Conditions
Content Creators

